The common name for the clavicle is the collar bone. This bone serves to cover and protect the brachial plexus, which is a structure made of several nerves that are responsible for the sensaton and motor function of each arm. The clavicle also acts as a strut that provides the only bony connection between upper limb (arm) and the thorax (chest). It is the first bone in the body to ossify (calcify) in a person’s early developmental stages.
Most people who have fractured their clavicle do not need surgery (Figure 1).
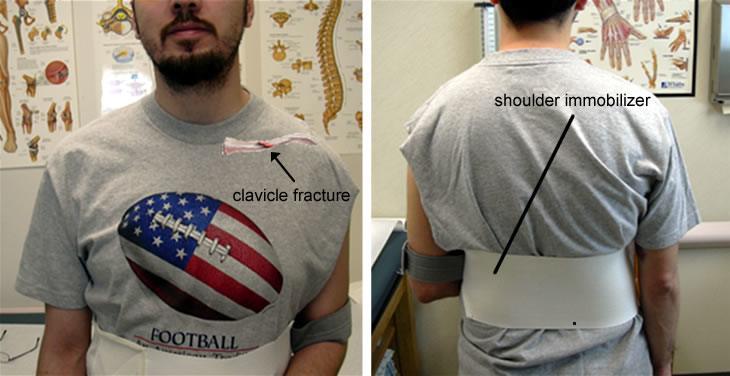
Figure 1. Conservative treatment of a clavicle fracture with a shoulder immobilizer. An arm sling or a figure-of-eight brace are also commonly used for nonsurgical treatment of this problem.
When an orthopaedic surgeon is evaluating a clavicle fracture he or she tries to classify the type of fracture into one of three groups.
Clavicle fracture classification
When an orthopaedic surgeon is evaluating a clavicle fracture he or she tries to classify the type of fracture into one of three groups:
- Group I: the clavicle is fractured in the middle of the bone. This is the most common region in which the clavicle is fractured in both adults and children, making up about 80% of all clavicle fractures. The medial bone fragment (the half of the bone next to the sternum) usually displaces upward due to the pull of the sternocleidomastoid muscle on that portion of the clavicle. The lateral fragment (the half of the bone that is toward the shoulder) is pulled downward by the weight of the arm.
- Group II: the clavicle is fractured at the distal third of the bone (toward the shoulder). This fracture pattern accounts for 10-15% of all clavicle fractures. Group II fractures may be subdivided into three separate types:
- Type 1: there is minimal displacement of the two ends of the bone
- Type 2: the fracture is medial to a group of ligaments called the coracoclavicular ligaments. These ligaments, along with the ligaments of the AC joint, connect the clavicle to the scapula.
- Type 3: the fracture involves the articular joint surface of the AC joint. Fractures that are this distal may have a high incidence of nonunion, meaning that the bone does not always heal properly to produce a solid, bony structure. Still, most nonunions are asymptomatic, and of these only a small number will be problematic enough to require surgery.
- Group III: the clavicle is fractured medially (close to the sternum). This is the least common location for a clavicle fracture, and accounts for only about 5% of all clavicular fractures
When treated nonoperatively, a patient will often wear a shoulder immobilizer, sling or a figure-of-eight brace for comfort while the bone heals (Figure 1). It is difficult to reduce and maintain the reduction of clavicle fractures; in other words, it is difficult to hold the two ends of the broken bone together in perfect alignment. Despite this, healing usually proceeds rapidly.
It is very common for the patient to be "left" with a prominent bump where the fracture has healed due to the bony callus that is produced during the healing process. Almost all patients do well functionally despite this bump. It may be possible to prevent formation of the bump by fixing the bone surgically with a plate and screws. However, this simply trades one cosmetic deformity (the prominent bump) for another (a surgical scar), and it subjects the patient to the risks associated with the anesthesia that must be administered in order to to perform the procedure.
A physician is likely to recommend surgery (Figure 2) when:
- the fracture is open, meaning that the bone has been exposed to the outside world through a wound. Your surgeon will most likely wash out the wound in the operating room, and he or she may then repair the bone using hardware (usually a plate and screws) at that time, or possibly during a subsequent wash-out procedure
- the sharp ends of the fractured bone cause tenting of the skin (in other words, the bone looks like it is going to pop through the skin)
- there is significant shortening of the bone due to overlapping of the two bone ends at the fracture site, which may cause medialization of the shoulder girdle
- the clavicle does not heal on its own after several months (this is called a nonunion)
- the patient has multiple injuries to other parts of the body and needs to use the affected upper extremity during the rehabilitation period.
- the clavicle fracture occurs as part of a floating shoulder injury
A floating shoulder variant. In this case, the ligaments appear to be intact, but there is a fracture of the clavicle and the scapular neck. This patient’s shoulder displaced after one week of conservative treatment in a sling, thus requiring surgical treatment.

Figure 2. Open reduction and internal fixation of a clavicle fracture with a plate and screws.